After a long time I've had the idea to get back to writing and this one is about how state capacity and the ability to write good legislation leads to wonderful outcomes. This story is from my personal experience building EHRs that needed barcode scanning to enter drugs to prevent errors in administration. If a barcode is scanned before administration then it can be validated against the prescription to make sure it's compliant. This was a requested feature for months on end and I had put it off since I assumed that we needed access to a proprietary dataset that contains barcode mappings to the product details. The other option was to have the inventory manager scan everything so that we maintain a log of all drugs, this is error prone and introduces a new change in their workflows. In India where I previously developed applications it was complicated and you usually contracted with a pharmacy chain to get access to this data.
Curiously while exploring options with Claude, it told me that all barcodes for drugs in the US have the National Drug Code encoded within them. This was new information to me. This meant that I could write a scanner using any barcode reader and interpret the barcodes using NDC which is free to download on the FDA's own site - National Drug Code Directory
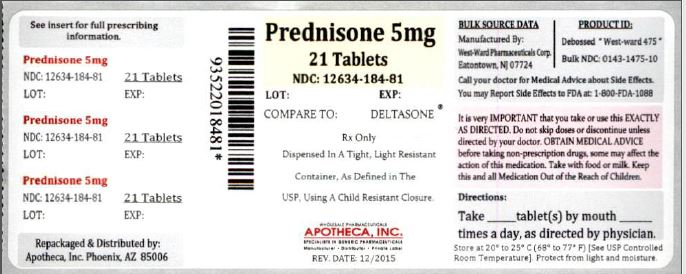
Example for Prednisone 5mg that shows Barcode 93520-18481 and corresponding NDC number as 12634-18481
At the top this seems like a normal feature of a country where the regulators want to make it easier for people to use the directories they build so that it increases patient safety. This is not the case in India, where the agency that approves drugs for human use and the agency responsible for making these datasets available aren't the same, leading to datasets that aren't accurate. As a business if you know the data you're getting isn't accurate you won't put it into use at all and this is the case with India's drug codes.
They'll even tell you in their release file that they don't want to cover all drugs.